Culture change

Policy slashes rates of baseless urine screening before hip or knee replacement surgery
Choose wisely: in hospitals it’s a mantra underpinned by evidence and motivated by concern for patients, resources and the health care system writ large. Much research has shown that some tests should not be ordered, either because the results will not influence the decisions made, or, worse, because they could do harm.
Sunnybrook’s Holland Centre does about 3,300 surgeries every year. Until May 2015, screens of urine cultures were routinely ordered before patients had their joints replaced. The thinking was that if the cultures tested positive for bacteria, then patients should be treated with antibiotics before having surgery to reduce the odds of getting a joint infection. The wrinkle in this thinking? “I’ve been doing joint replacements for over 30 years. I don’t think I’ve ever had a patient develop an acute postoperative infection from a urinary organism,” says Dr. Jeff Gollish, medical director of the Holland Centre.
Added to a lifetime of surgical experience are data—or a lack thereof. “We have not had prospective studies demonstrating that if you [order urine cultures and find bacteria] and then treat the urine that you can reduce the risk of infection in the joint replacement surgery,” says Dr. Jerome Leis, medical director of infection prevention and control at Sunnybrook, and an associate scientist at Sunnybrook Research Institute.
Thus Leis and Gollish were prompted to figure out how to change practice. Education, they surmised, wasn’t enough. “What we did was slightly different; we implemented a system change,” says Leis. They developed a policy such that urine screening was not done automatically. They removed it from the standard set of tests ordered before surgery. For specimens received by the lab there was “a little bit of a hard stop,” says Leis. “The lab upon receipt of the specimens would not automatically process them.” Instead, anyone who wanted the culture done had to call the lab to request it within 24 hours.
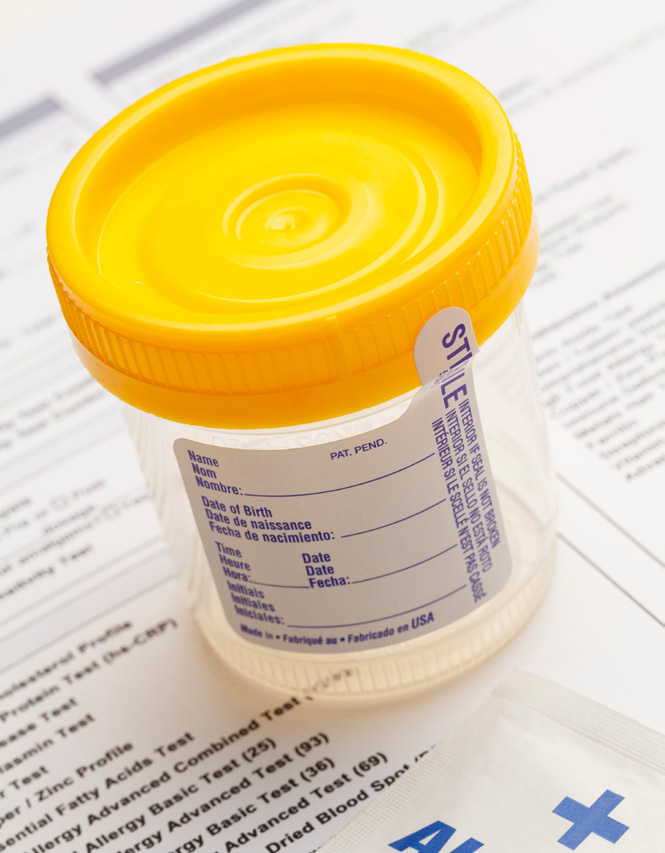
After launching a policy change, routine ordering of unwarranted urine cultures before joint replacement surgery dropped.
Photo: PixelRobot / Depositphotos.com
As detailed in a March 2017 article in Clinical Infectious Diseases, it worked. The researchers evaluated 3,523 patients undergoing a first total knee, hip or shoulder replacement during two years leading up to the policy change. They compared them to 1,891 patients who had surgery after the policy change. Before the change, 3,069 screening urine cultures were ordered over the two years, all of which were processed; of these, 352 were positive. After the change, 126 cultures were ordered, only 10 of which were processed; none were positive. This corresponded to a 99% relative reduction in the screening rate of urine cultures. “The system change led to a dramatic shift in practice, and not only dramatic, but rapid—within a month,” says Leis.
They also found no significant year-over-year increase in joint infections after the change. “In fact, among those that we did find, they were caused by bacteria that do not originate from the urinary tract, suggesting they were unrelated to this change in the intervention,” says Leis.
The results also have societal reverberations. “Antibiotic stewardship and avoiding inappropriate use of antibiotics is critical to avoid developing organisms for which we have no treatment,” says Gollish. “We are starting to see the development of multi-drug-resistant bacteria where we have limited treatment options, and anything we can do to scale back unnecessary antibiotics is essential,” Leis says.
Gollish notes that while it is standard practice at the Holland Centre not to order urine cultures unless patients have symptoms that warrant testing, this isn’t the case elsewhere. “If I talk to my colleagues across the country, virtually everybody is still doing this in most hospitals.” He hopes to move the change into wider use through his work with the National Standards Committee of the Canadian Orthopaedic Association.
Working to achieve consensus on the change was pivotal to success. “This is an example of what we can accomplish when we collaborate between clinical services, including orthopaedics, infectious diseases, infection control, antimicrobial stewardship and microbiology,” says Leis, then adds, “by all being at the table and coming up with a process that everyone agrees on and acknowledges is a better use of resources, we can make system changes that are more impactful and sustainable.”
— Stephanie Roberts

